Introduction
Heart failure (HF) is a common, progressive clinical syndrome associated with substantial morbidity, premature mortality and high healthcare utilisation. In the UK, approximately one million people are currently living with HF, with five-year mortality approaching 50%. Despite advances in pharmacological and device therapies, many patients continue to experience delayed assessments, recurrent hospitalisation and poor long-term outcomes. As prevalence continues to rise due to an ageing population, increasing multimorbidity and improved survival from cardiovascular disease, demand on specialist heart failure, cardiology and echocardiography services has increased significantly. Cardiac physiologist/clinical scientist-led heart failure echocardiography surveillance clinics (P/SLSC) have the potential to improve pathway efficiency, support specialist HF services and increase consultant capacity by delivering protocolised follow-up, advanced imaging assessment and surveillance within agreed governance frameworks.
A clinical scientist/cardiac physiologist HF surveillance clinic will:
- Support timely surveillance of diagnosed HF patients
- Provide advanced echocardiographic assessment and interpretation
- Support HF multidisciplinary team (MDT) decision-making
- Identify patients requiring escalation for specialist review
- Improve efficiency of imaging-led HF pathways
- Standardise surveillance and imaging protocols
- Contribute to quality improvement, audit and pathway optimisation
Indications and referral
Inclusion
Physiologist/scientist-led heart failure follow-up clinics are intended for clinically stable patients with an established diagnosis of HF who require protocolised surveillance and imaging follow-up within a specialist HF pathway. Patients suitable for review within the P/SLSC must have undergone prior assessment and management planning by a heart failure consultant or specialist HF MDT. Referral to the P/SLSC must originate from a HF consultant, specialist HF service or agreed local HF pathway.
The scope of clinical practice will include patients with:
- Cardio-oncology:
- Serial LV function monitoring (including global longitudinal strain)
- Early detection of Chemotherapy-Induced Cardiac dysfunction
- Collaboration with oncology teams and cardio-oncologist
- Post MI:
- Pre-discharge EF <35%: Ensuring referral to community HFNS with echo/meds review at 3 months on optimal medical therapy for consideration of device implant
- Pre-discharge EF 35-45%: Protocol for 6-week HF echo physiologist review provided referral form including checklist for discharging clinician regarding prescribing status of ACE-/BB/MRA and sglt2- (Discharging clinician to indicate next to each: Yes/Not indicated/No - contraindication/exclusion). Repeat echo to assess whether recovery of EF or whether referral to HF services is required
- Device requirement assessment protocols:
- FU of known HF patients on optimal medical therapy with LBBB and impaired EF to (or D/W consultant to) refer for CRTP/D if EF falls <35%
- FU of HF patients 3 months after medical optimisation for EF/referral for ICD where appropriate
- CRT optimisation clinic:
- Screening post CRT patients suitable for assessment (non-response/low pacing %/PNS). Checking symptoms/signs and medications + observations. Acquire images. Generate draft plan for consultant review with pacing scientist / physiologist
- Inpatient HF team support:
- VexUS plus LUS plus IVC US for difficult fluid balance assessment (ie nephrotic syndrome). Urgent high-quality images where required to inform urgent decision making. Flag up in-patients with new finding of LVSD (or other relevant findings as appropriate to service) to in-reach inpatient HF team. Support inpatient team in challenging diagnoses such as suspected infiltrative disease
Exemptions
The following exemptions apply to a P/SLSC:
- Patients requiring specialist assessment for the diagnosis of heart failure (regardless of ejection fraction - see appendix 1 for more details).
- Patient requiring specialist assessment for end-of-life care.
- Request reason(s) deemed inappropriate by consultant cardiologist.
- Unwell patients (clinical features/disease processes at the discretion of a cardiologist).
- Pregnant patient.
- Poor echo imaging that prevents accurate and reliable surveillance.
- Patients under the age of 16 years.
- Patients who refuse to be seen in the P/SLSC or lack capacity for independent decision making.
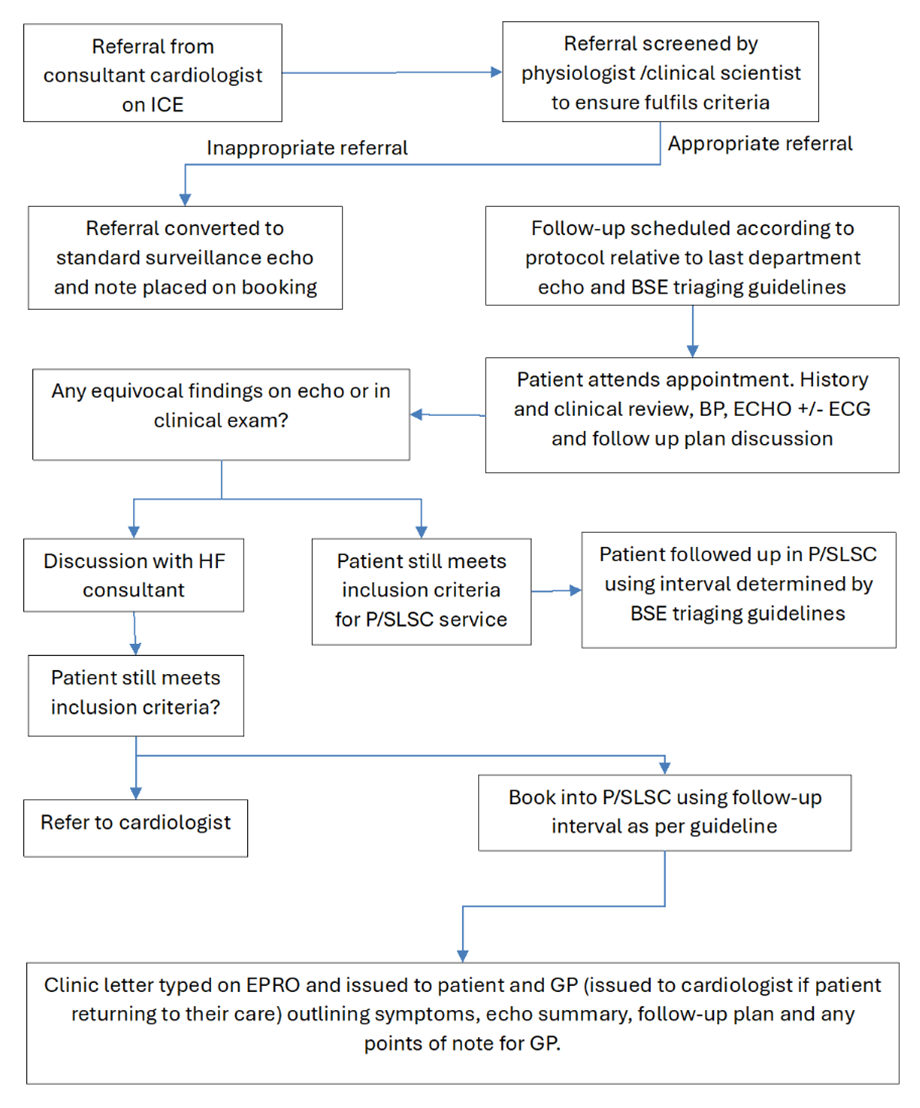
Performing the P/SLSC
P/SLSC staff will introduce themselves and their job title in a way that is clear and understood. The patient will enter the echo lab where the scientist/physiologist will perform a clinical history, brief examination, BP measure, and TTE in compliance with BSE guidelines. At the end of the appointment, the patient is notified of the result and follow up plan. Red flag symptoms will be identified to the patient. P/SLSC staff will compose a letter to the patient and GP summarising the outcome and result of the appointment. For equivocal findings requiring further review, the patient will be notified that their case will be discussed with the consultant responsible for their overall care and that their letter will explain the decisions made.
Report and interpretation
- The report will be performed on the standard department TTE reporting software and will be uploaded into the patient medical records according to local service practice
- A clinic letter will be produced according to the P/SLSC letter template and sent to both the patient and their GP
- Interpretation of the echocardiographic and clinical findings will be performed by the cardiac scientist/physiologist. BSE reporting guidelines, national/international HF management guidelines, and local service policy will help inform follow-up plans and surveillance timeframes
- Patients who no longer meet the requirements for P/SLSC surveillance will return to the care of the initial referring cardiologist. This will be communicated to the patient during the S/PLHFC appointment and will be detailed in the patient/GP letter with a copy/referral sent to the cardiologist
- Equivocal / inconclusive findings will be discussed with an HF cardiologist or P/SLSC clinical lead at the local HF MDT to determine next action. Time should be dedicated each week for the scientist/physiologist to present and discuss cases with the S/PLHFC clinical lead
- Follow-up appointments should be requested and scheduled according to local service policy
Appendix 1
This accreditation does not confer independent clinical practice.
A Level 3 echocardiographer contributes advanced diagnostic expertise to support clinical decision-making. Recommendations regarding treatment and referrals to specialist services, including device teams, should be made within a multidisciplinary framework, ensuring that patient management decisions are appropriately discussed and agreed at MDT level.
Practice should take place within documented governance arrangements, including:
- named supervising HF consultant(s)
- regular participation in HF MDT meetings, and
- ongoing HF-specific continuing professional development in addition to echocardiography requirements
What is out of scope for a scientist-/physiologist-led heart failure clinic?
- The British Society for Heart Failure align with NICE HF guidance in the requirement for specialist assessment for HF diagnosis and do not recommend this as a task for the Level 3 accredited echocardiography scientist/physiologist
- Referral for end-of-life services requires wider consideration by the HF specialist team and is not suitable for the Level 3 trained echocardiography scientist/physiologist. Potential cases may be referred/presented at the HF MDT
The underlying rationale for this is:
- HF is an extreme high-risk condition. CPRD (UK) data shows that in the intermediate group (NT-proBNP 400-2000ng/l), 1 in 5 patients will have died by 12 months. In the higher-risk group (NT-proBNP >2000ng/l) more than 1 in 4 patients have died by 12 months
- NT-proBNP is non-specific test for HF but is an excellent prognostic marker, particularly for death. Excluding HF on echo is insufficient, as raised NT-proBNP indicates that the patient is at risk and the likely alternative cause(s) must be identified and addressed promptly
- 90% of HF patients are multi-morbid, so the holistic management plan requires optimisation of multiple other co-morbidities plus medication rationalisation and good clinical care extends beyond cardiology, requiring additional general medical and expertise
- HF with preserved ejection fraction (HFpEF) in particular is a diagnosis of exclusion. Multiple non-cardiac causes must be excluded before attributing symptoms/clinical signs to the subtle and common echocardiographic abnormalities associated with HFpEF
- HF patients are complex and are particularly unstable at the point of diagnosis and discharge after a HF admission. The patient’s trajectory can change rapidly. The specialist or specialist MDT responsible for the patient’s management plan must be contactable by the HFNS teams for ongoing advice when the patient deteriorates
- In addition to confirmation of diagnosis, the initial HF assessment also requires identification of the underlying aetiology with additional investigations depending on the clinical scenario plus specific directed treatment as required