Introduction
Current evidence predicts that by 2050, over 6.5million new cases of valvular heart disease (VHD) will be diagnosed in Europe¹ alone. In the UK, there are currently over 1 million patients over the age of 65 living with VHD, with this number expected to increase by 50% in less than 10 years¹; the requirement of pre-intervention surveillance and post-operative follow-up for this growing population significantly increases the demand on both cardiology and echocardiography services. However, current evidence indicates that follow-up for patients with VHD is often performed by non-specialist cardiologists and is poorly standardised³. In line with national GIRFT recommendations, increasing numbers of specialist cardiac physiologist/clinical scientist-led follow-up clinics (P/SLVC) have been established and have reduced both the number of patient hospital appointments and the number of echocardiograms being performed, whilst adhering to management guidelines and maintaining patient outcomes.
A clinical scientist/cardiac physiologist valve surveillance clinic will:
- Standardise care through a singular surveillance/follow-up pathway
- Adhere to current national guidelines and simultaneously prevent delays in surveillance/care and unnecessary/too frequent call-back
- Ensure timely referral for consultant review on development of severe valve disease or symptoms
Indications and referral
Inclusion
All patients entering surveillance within the P/SLVC must be free from cardiac symptoms and must have been deemed suitable for referral following clinical review by a consultant cardiologist or specialist registrar. The scope of clinical practice will include patients with:
- Morphologically normal or congenitally abnormal native valves with less than severe disease
- Bicuspid aortic valve with non-dilated and structurally normal aorta
- Valve lesion as above with dilated aortic root or proximal ascending aorta but ≤4.0cm without connective tissue disease or bicuspid aortic valve
- Normal functioning replacement or repaired valves
- Mild or moderate but stable prosthetic/repaired valve dysfunction
Exemptions
The following exemptions apply to a P/SLVC:
- Request reason(s) deemed inappropriate by consultant cardiologist
- Unwell patients (clinical features/disease processes at the discretion of a cardiologist)
- Pregnant patient
- Poor echo imaging that prevents accurate and reliable surveillance
- Patients under the age of 16 years
- Patients who refuse to be seen in the P/SLVC or lack capacity for independent decision making
- Symptoms or pathology requiring intervention, including but not limited to: chest pain with coronary artery disease; symptoms of heart failure (irrespective of LVEF), unstable or new arrhythmias
- Patients with severe native valvular disease
- Patients with complex congenital VHD, including the Ross procedure
- Patients with VHD in association with connective tissue disorders including: Marfan’s, Ehlers Danlos and Lois Dietz
- Patients who have VHD with pulmonary hypertension (Pulmonary artery systolic pressure 35mmHg or above)
- Patients with a LVEF <50% irrespective of heart failure status/symptoms
- Poor prognosis, significant co-morbidities, or patients under palliative care
Referral
- Referral may happen at any time following the initial clinical review or during follow-up consultations
- Requests will be vetted according to the inclusion/exemption criteria
- Identification and management of referrals will be in-line with local trust scheduling systems
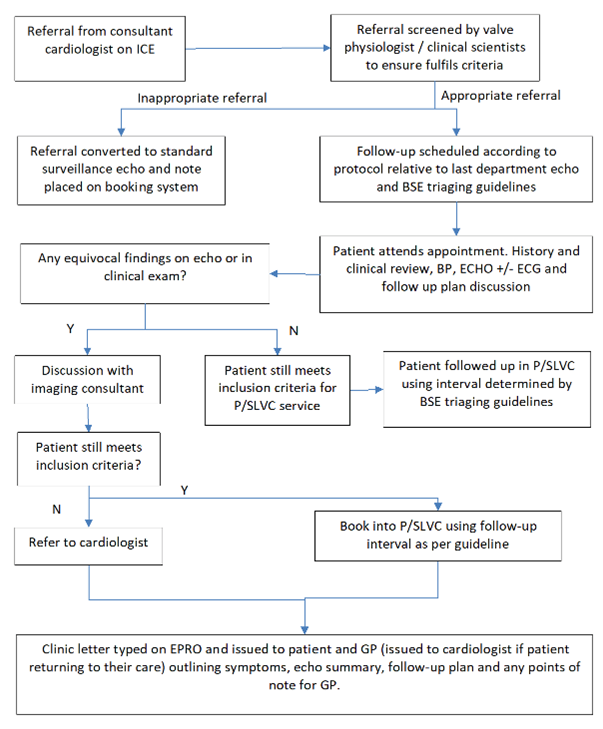
Performing the P/SLVC
P/SLVC staff will introduce themselves and their job title in a way that is clear and understood. The patient will enter the echo lab where the physiologist/scientist will perform a clinical history, brief examination, BP measure, and TTE in compliance with BSE guidelines. At the end of the appointment, the patient is notified of the result and follow up plan. Red flag symptoms will be identified to the patient and hypertension advice given if the BP recording is high. P/SLVC staff will compose a letter to the patient and GP summarising the outcome and result of the appointment. For equivocal findings requiring further review, the patient will be notified that their case will be discussed with the consultant responsible for their overall care and that their letter will explain the decisions made.
Report and interpretation
- The report will be performed on the standard department TTE reporting software and will be uploaded into the patient medical records according to local service practice
- A clinic letter will be produced according to the P/SLVC letter template and sent to both the patient and their GP
- Interpretation of the echocardiographic and clinical findings will be performed by the cardiac scientist. BSE valvular guidelines, national/international valve management guidelines, and local service policy will help inform follow-up plans and surveillance timeframes
- Patients who no longer meet the requirements for P/SLVC surveillance will return to the care of the initial referring cardiologist. This will be communicated to the patient during the P/SLVC appointment and will be detailed in the patient/GP letter with a copy/referral sent to the cardiologist
- Equivocal / inconclusive findings will be discussed with an imaging cardiologist or S/PLVC clinical lead at an echo MDT to determine next action. Time should be dedicated each week for the scientist/physiologist to present and discuss cases with the P/SLVC clinical lea
- Follow-up appointments should be requested and scheduled according to local service policy