Introduction
Inherited cardiac conditions (ICCs) are a broad group of familial conditions that affect the heart muscle or electrical system. They include inherited disorders of:
- Heart muscle (cardiomyopathies)
- Ion channels (channelopathies)
- Great vessels (aortopathies)
- Skeletal and cardiac muscle (neuromuscular conditions)
Hypertrophic cardiomyopathy (HCM) and dilated cardiomyopathy (DCM) are the most common ICC’s that affect the heart muscle, with a HCM prevalence of approximately 1|:200 to 1:500 and DCM around 1:250 to 1:1000. Most ICCs follow an autosomal dominant inheritance pattern, resulting in a 50% chance of a gene-carrier parent passing the condition to each of their children. Although the overall annual risk of sudden cardiac death (SCD) varies by condition, ICCs account for a high percentage of SCD cases in individuals under the age of 35. However, penetrance and expressivity vary widely. Many mutation carriers live normal, asymptomatic lives, while others may experience severe heart failure, life-threatening arrhythmias, and death. Screening clinics in first-degree relatives of ICC probands are therefore essential for early diagnosis and initiation of appropriate management plans.
Cardiac physiologists / clinical scientists are an instrumental part of the ICC team, delivering the key diagnostic investigations of transthoracic echocardiograms (TTE) and 12-ECG that are critical in the diagnosis, management, and screening of ICCs. By utilising advanced skills and training, S/PLSC have the potential to offer a one-stop screening service, generating additional consultant capacity for follow-up of high-risk patients with established cardiomyopathy diagnoses.
A cardiac physiologist/clinical scientist ICC surveillance clinic (P/SLSC) will:
- Standardise care through a singular surveillance/follow-up pathway
- Adhere to current national guidelines and simultaneously prevent delays in surveillance/care and unnecessary/too frequent call-back.
- Ensure timely referral for consultant review on development of ICC condition or symptoms
Indications and referral
Inclusion
All patients entering the P/SLSC clinic must have been deemed suitable for referral following review by a consultant cardiologist or specialist registrar. The scope of clinical practice will include patients with:
- First-degree relatives of patients with a confirmed diagnosis of HCM or DCM
- Patients who have undergone a full diagnostic screening and clinical review by an ICC specialist consultant with no clinical, ECG, or echocardiographic features suggestive of the ICC under investigation but in whom, ongoing surveillance is required
Exemptions
The following exemptions apply to a P/SLSC:
- Request reason(s) deemed inappropriate by consultant cardiologist
- Unwell patients (clinical features/disease processes at the discretion of a cardiologist)
- Pregnant patient
- Poor echo imaging that prevents accurate and reliable surveillance
- Patients under the age of 16 years
- Patients who refuse to be seen in the P/SLVC or lack capacity for independent decision making
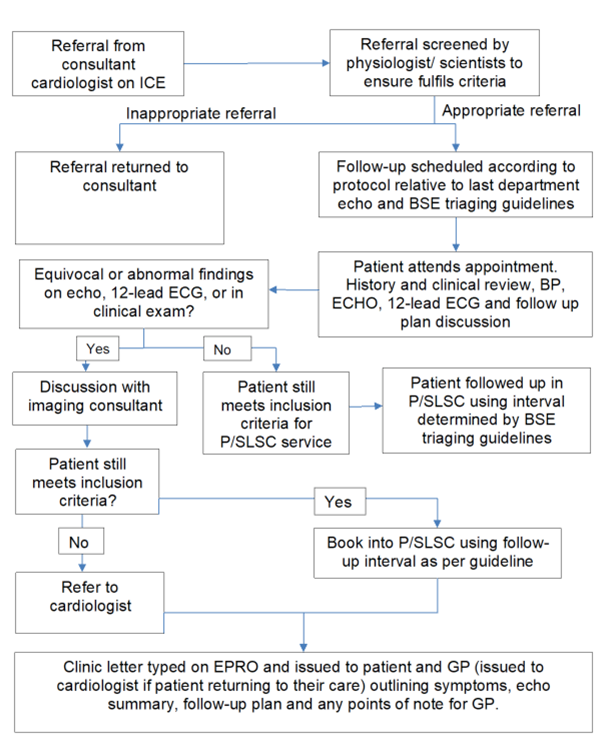
Performing the P/SLSC
P/SLSC staff will introduce themselves and their job title in a way that is clear and understood. The patient will enter the echo lab where the scientist/physiologist will perform a clinical history, brief examination, BP measure, and TTE in compliance with BSE guidelines; the 12-lead ECG can be performed before or after the study but will be reviewed alongside all other findings. At the end of the appointment, the patient is notified of the result and follow up plan. Red flag symptoms will be identified to the patient for awareness. P/SLSC staff will compose a letter to the patient and GP summarising the outcome and result of the appointment. For equivocal findings requiring further review, the patient will be notified that their case will be discussed with the consultant responsible for their overall care and that their letter will explain the decisions made.
Escalation
All P/SLSC should have ICC consultant oversight. If medical advice is required at any stage in the screening process, the following ways of seeking help are available:
- ICC consultants can be contacted directly via telephone for urgent medical queries
- For non-urgent clinical questions or advice, the case can be discussed at either an imaging MDT or during in-person case-review
- Informal, ad-hoc advice should always available
- Patients can be booked in to see a consultant for follow up directly
Report and interpretation
The report will be performed on the standard department TTE reporting software and will be uploaded into the patient medical records according to local service practice
- A clinic letter will be produced according to the P/SLSC letter template and sent to both the patient and their GP
- Interpretation of the echocardiographic and clinical findings will be performed by the cardiac scientist/physiologist. BSE guidelines, national/international management guidelines, and local service policy will help inform follow-up plans and surveillance timeframes
- Patients who no longer meet the requirements for P/SLSC surveillance will return to the care of the initial referring cardiologist. This will be communicated to the patient during the P/SLSC appointment and will be detailed in the patient/GP letter with a copy/referral sent to the cardiologist
- Equivocal / inconclusive findings will be discussed with an imaging cardiologist or P/SLSC clinical lead at an echo MDT to determine next action. Time should be dedicated each week for the physiologist/scientist to present and discuss cases with the P/SLSC clinical lead
- Follow-up appointments should be requested and scheduled according to local service policy