The volume and complexity of structural heart interventions is rapidly expanding, and currently the majority are performed with transoesophageal echocardiography guidance by an interventional echocardiographer (IE).
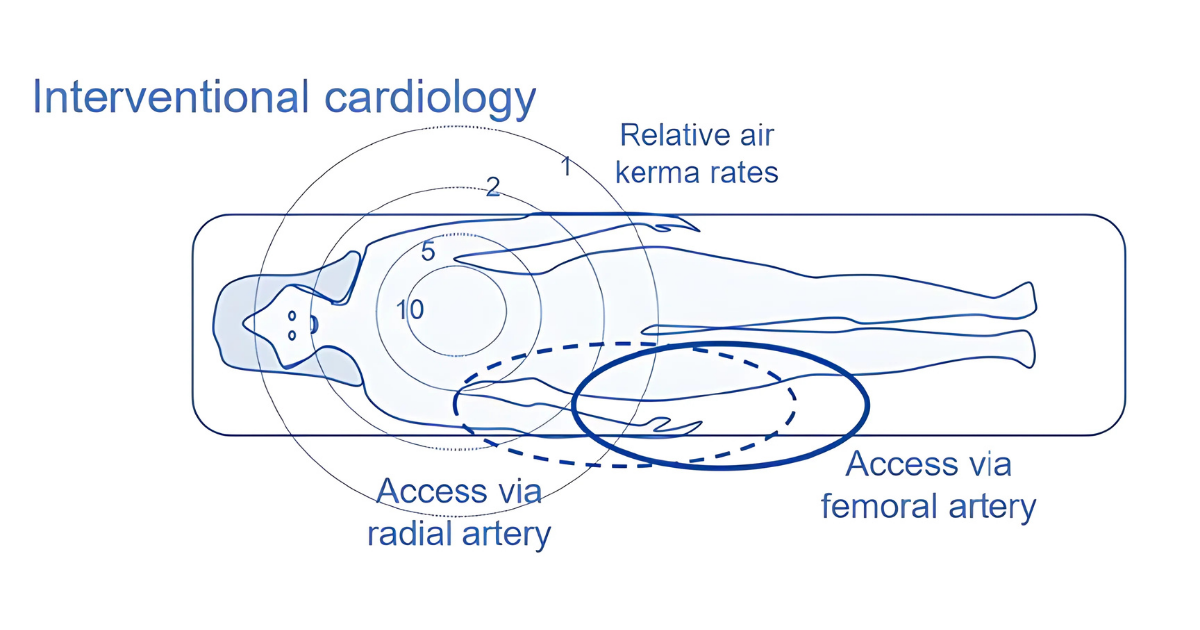
Studies comparing the radiation exposure of the interventional cardiologist and IE have demonstrated a 3 to 10-fold higher radiation exposure to the IE1,2, 3. This is not surprising since the TOE operator typically stands nearest the radiation source with the highest exposure to the hand, waist and lower body4. Radiation exposure will vary depending on procedural complexity, fluoroscopy time and C arm angles and studies have shown radiation exposure to be associated with cancers, cataracts, hypertension, hyperlipidaemia and endothelial dysfunction5.
A recent European Association of Cardiovascular Imaging (EACVI) survey on radiation exposure in interventional echocardiography highlighted the wide variation in the provision of radioprotection devices across Europe6. Despite the internationally agreed ALARA (as low as reasonably achievable) standard, the burden of exposure remains poorly recognised5.
Several publications have sought to educate the IE in understanding the risks and the necessary mitigating measures. The three key principles are limiting the duration of exposure, increasing the distance from the X-ray source, and shielding all operators with effective protective clothing7.
Employers have a duty of care to workers who are exposed to ionising radiation and should provide the correct radiation clothing and shield protection equipment8. The British Society of Echocardiography (BSE) recommend that interventional echocardiography should be provided with the following as a minimum standard of protection, training, and monitoring:
Shielding and distance
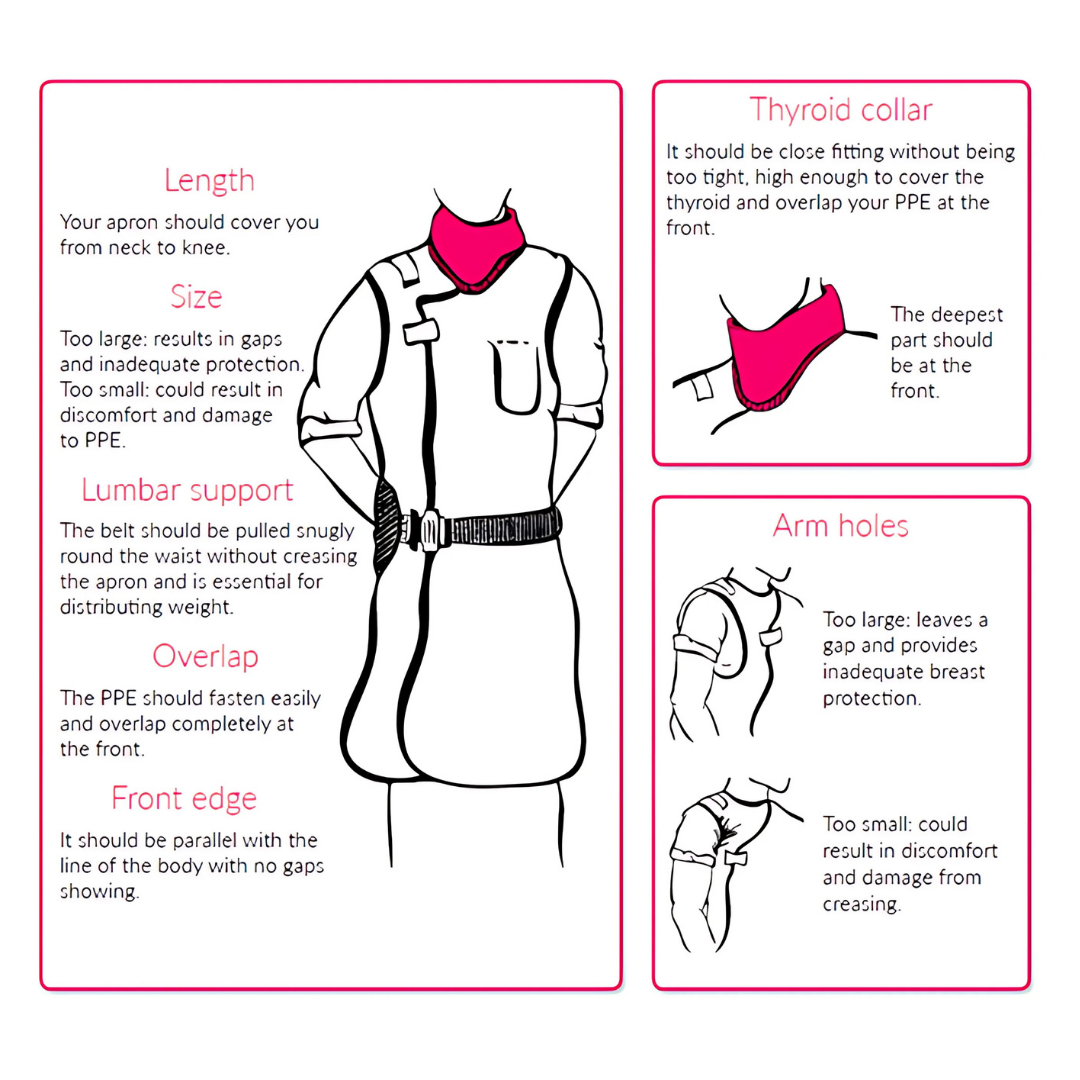
- Well maintained and appropriately fitting lead protection with two-piece designs preferable to single long aprons and including thyroid collars.
- Lead apron should be wrap around style and ³0.25mm lead thickness thereby by providing minimum 50mm lead thickness to the side facing the X-ray source.
- Regardless of the design, it is crucial that the lead protection fits properly at the neckline and armhole. Large gaps could result in the increased exposure of breast tissue, which is especially important for female staff.
- Provision of axillary protection for all female operators, such as a sleeve, wing, or axillary supplement, to provide protection to breast tissue.
- A thyroid collar should be worn appropriately to minimise any gaps above the lead apron.
- Provision of lead glasses, at least 0.75mm or equivalence - with prescription lenses if required - to be worn by the TOE operator during procedures.
- Availability of shielded gloves and arm sleeves to be worn depending on operator preference
- Adjustable lead shielding on both under sides of the catheter lab table (rather than the interventional operator side only) to reduce scatter radiation.
- Dedicated additional shielding equipment between the TOE operator, the X-ray source and patient is necessary since the highest exposure is at the waist and lower limbs. A combination of ceiling mounted and moveable floor standing screens to allow for variation in operator and machine position is preferable.
- The IE should position themselves as far away from the C-arm as possible especially during fluoroscopy or cine acquisition.
Exposure time and communication
- Time for image acquisition should be minimised.
- If formal cine-acquisition is required, then the interventional echocardiographer should be informed and allowed to rest the TOE probe on the table and stand well back.
- Procedures utilizing the C-arm in a right anterior oblique (RAO) position supply the most radiation exposure to the interventional echocardiographer. Left atrial appendage occlusion and tricuspid transcatheter interventions often require RAO positions as does the cusp-overlap view in some TAVI procedures.
- Use of this C- arm position should be minimised or if required should be clearly communicated to the IE. The IE should consider resting the TOE probe on the table and to stand back during RAO projections for prolonged fluoroscopy or cine-acquisition.
Training and monitoring
- Institution hosted training in radioprotection and periodic certification including IRMER regulations to ensure knowledge and compliance analogous to interventional cardiologists.
- Personalised dose monitoring with wearable dosimetry devices including rings to monitor hand doses and glass badges for eye doses with regular audit of dose received.
- Provision of a slave fluoroscopy monitor to facilitate viewing of the live fluoroscopy to assist in following and guiding the intervention and reduce the need to move closer to the X-ray source to view images and be aware when X-ray screening is occurring.
- Wider education of the whole heart team will be crucial for mitigating radiation risks to the IE. Interventional cardiologists must try to limit fluoroscopy time (e.g. utilising pre-procedural CT planning for optimal angles and reliance on peri-procedural TOE guidance), minimise radiation dose during acquisitions and limit the use of adverse C-arm projections.
- Implementation of innovative technologies such as real time dosimetry and advanced shielding with real time feedback to enhance awareness and prompt behavioural adjustments9.
The BSE will commission a survey of current practice across UK structural heart intervention centres to provide national data on the activity and extent of protection and training currently provided.
 |
|
Figure 1. How the radiation dose varies with operator position for interventional cardiology10
|
 |
|
Figure 2. Example of additional shielding and slave fluoro monitor for the TOE operator
|
 |
|
Figure 3. Wearing your PPE11
|
 |
|
Figure 4. An operator wearing additional axillary lead protection9
|
*Data supporting the use of head protection is limited and therefore is optional although scatter radiation from the X-ray source may result in exposure to the upper body and head highlighting the importance of dedicated additional shielding equipment
BSE Council and Trustees July 2025, with thanks to Jim Newton, Sushma Rekhraj, Bushra Rana, Medhi Eskandari, Nilesh Sutaria, Dominik Schlosshan, Rick Steeds and Alexandra Thompson
Endorsed by:


References
The references for this guidance were published incorrectly in a previous version and updated on 18/08/2025. The British Society of Echocardiography apologises for any inconvenience caused.
- Kataoka A, Takata T, Yanagawa A, Kito K, Arakawa M, Ishibashi R, Katayama T, Mitsui M, Nagura F, Kawashima H, Hioki H, Watanabe Y, Kozuma K, Kotoku J. Body Surface Radiation Exposure in Interventional Echocardiographers During Structural Heart Disease Procedures.
JACC Asia. 2023 Mar 28;3(2):301-309. doi: 10.1016/j.jacasi.2022.12.008. eCollection 2023 Apr. PMID: 37181397
- McNamara DA, Chopra R, Decker JM, et al. Comparison of Radiation Exposure Among Interventional Echocardiographers, Interventional Cardiologists, and Sonographers During Percutaneous Structural Heart Interventions. JAMA Netw Open. 2022;5(7):e2220597. doi:10.1001/jamanetworkopen.2022.20597
- Crowhurst JA, Scalia GM, Whitby M, Murdoch D, Robinson BJ, Turner A, Johnston L, Margale S, Natani S, Clarke A, Burstow DJ, Raffel OC, Walters DL. Radiation Exposure of Operators Performing Transesophageal Echocardiography During Percutaneous Structural Cardiac Interventions. J Am Coll Cardiol. 2018 Mar 20;71(11):1246-1254. doi: 10.1016/j.jacc.2018.01.024. PMID: 29544609.
- Salaun E, Carles S, Bigand E, Pankert M, Aldebert P, Jaussaud N, Theron A, Cuisset T, Lambert M, Grisoli D, Franceschi F, Avierinos JF, Collart F, Deharo JC, Bonnet JL, Habib G. High Radiation Exposure of the Imaging Specialist During Structural Heart Interventions With Echocardiographic Guidance. JACC Cardiovasc Interv. 2017 Mar 27;10(6):626-627. doi: 10.1016/j.jcin.2017.01.016. PMID: 28335903
- Garcia-Sayan E, Jain R, Wessly P, Mackensen GB, Johnson B, Quader N. Radiation Exposure to the Interventional Echocardiographers and Sonographers: A Call to Action. J Am Soc Echocardiogr. 2024 Jul;37(7):698-705. doi: 10.1016/j.echo.2024.03.002. Epub 2024 Mar 13. PMID: 38490315
- E Galli, H Soliman-Aboumarie, L Gargani, P Szymański, A Gimelli, S E Petersen, L E Sade, I Stankovic, E Donal, B Cosyns, E Agricola, M R Dweck, N Ajmone Marsan, V Delgado, D Muraru, EACVI survey on radiation exposure in interventional echocardiography, European Heart Journal - Cardiovascular Imaging, Volume 25, Issue 6, June 2024, Pages 727–734, https://doi.org/10.1093/ehjci/jeae086
- Pilkington I, Sevenoaks H, James E, Eastwood D. Protecting female healthworkers from ionising radiation at work. BMJ. 2023 Apr 12;381:e075406. doi: 10.1136/bmj-2023-075406. PMID: 37045449
- Department of Health. Guidance to the Ionising Radiation (Medical Exposure) Regulations 2017. London: Department of Health; 2017.
- Modarai B, Haulon S, Ainsbury E, Böckler D, Vano-Carruana E, Dawson J, Farber M, Van Herzeele I, Hertault A, van Herwaarden J, Patel A, Wanhainen A, Weiss S, Esvs Guidelines Committee, Bastos Gonçalves F, Björck M, Chakfé N, de Borst GJ, Coscas R, Dias NV, Dick F, Hinchliffe RJ, Kakkos SK, Koncar IB, Kolh P, Lindholt JS, Trimarchi S, Tulamo R, Twine CP, Vermassen F, Document Reviewers, Bacher K, Brountzos E, Fanelli F, Fidalgo Domingos LA, Gargiulo M, Mani K, Mastracci TM, Maurel B, Morgan RA, Schneider P. Editor's Choice - European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on Radiation Safety. Eur J Vasc Endovasc Surg. 2023 Feb;65(2):171-222. doi: 10.1016/j.ejvs.2022.09.005. Epub 2022 Sep 18. PMID: 36130680
- Committee on Medical Aspects of Radiation in the Environment (COMARE). Nineteenth report: medical radiation – research and methodology. London: COMARE; 2022.
- British Institute of Radiology. How to wear a lead apron[Internet]. London: BIR; [date unknown] [cited 2025 Jun 25]. Available from: https://www.bir.org.uk/media/533937/advice_sheet_4_how_to_wear_a_lead_apron.pdf
Further resources